Your COVID-19 questions answered
We assembled our experts to offer responses to some of the most pressing questions regarding the current state of the pandemic. From the startling emergence of the Omicron variant to the use of rapid antigen tests to the recommendation and timing of third dose booster vaccines. The evidence collected by CITF-funded research so far has helped to inform health care and public health decisions with regard to the ever-changing situation. We hope that it will help you to make informed choices regarding your health and to stay safe.
At-home rapid antigen tests for COVID-19 have become more commonplace in the absence of widespread PCR testing. They are called antigen tests because they detect antigens, specific proteins that make-up the SARS-CoV-2 virus. Further, they provide test results in less than an hour, hence the designation ‘rapid’.
A rapid antigen test’s sensitivity, defined as its ability to detect the virus when present, is dependent on an individual’s viral load. Viral loads – the amount of virus in nasopharyngeal fluids and blood – are higher early on in infection when the virus is replicating exponentially4. Viral loads are generally detectable for some rapid antigen tests during the first five days of symptoms (Health Canada). After this initial period, rapid antigen test performance decreases quickly as viral loads decline, and the infection clears.
Rapid antigen tests detect current infections, including those caused by Omicron5. They cannot, however, tell whether an individual has had a previous infection with SARS-CoV-2. Vaccination against COVID-19 does not interfere with the test’s ability to detect a current infection.
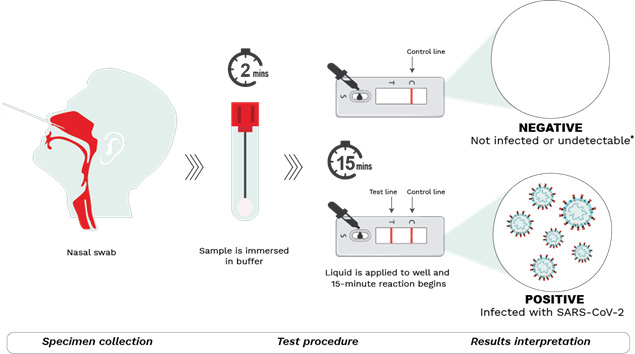
Figure 1: Schematic depiction of the COVID-19 rapid antigen tests available in Canada.
Step 1 – Specimen collection.
A nasal sample is collected using the sterile swab provided. Blowing the nose prior to swabbing, tilting the head back 70 degrees, compressing the nostril with the aid of fingers, and using circular motions while in the nasal cavity have been known to aid with collection.
Step 2 – Test procedure.
The swab is submerged in a buffer solution to extract the SARS-CoV-2 virus (if present). After a rest period, the resulting liquid is dispensed with the aid of a nozzle into the sample well on the testing device. The sample then moves through the testing device during which antigens present in the sample bind to antibodies in the device, forming antigen-antibody complexes. The reaction lasts for 15-30 minutes (depending on the manufacturer’s instructions) after which results may be read.
Step 3 – Results interpretation.
Two lines detected at the T (test) and C (control) lines of the test window indicate a positive result. This means the sample is positive for SARS-CoV-2 and the person is most likely infected. Positive results can be reported at local/provincial/territorial Public Health units or at independent initiatives such as The Rapid Test Tracker. If only one line at C (control) appears, the result is negative, meaning that the individual is most likely not infected. *It is important to note however that a negative result may also indicate that a person is infected but below the level of detection. That said, if symptoms are present, individuals should continue to isolate and follow local public health guidelines. The test may be repeated a few days later to re-ascertain infection status. No lines or a faint T line indicates an invalid test. A test cannot be used more than once.
Some of the rapid antigen tests that have received Health Canada approval for diagnostic testing are shown below, and additional information can be found here.
Table 1: Specifications of some of the rapid antigen tests available in Canada.
| Country of manufacture | Sensitivity* | Specificity** | Overall agreement*** | Limit of detection | |
| BTNX – Rapid Response COVID-19 Antigen Test | Canada | 95.5% | 95.5% | 97.3% | 2×102.4 TCID50/mL |
| Artron Antigen COVID-19 (SARS-CoV-2) Rapid Test | Canada | 97.2% | 99.6% | 97.0% | 1×103
TCID50/mL |
| Quidel Quickvue At-home OTC COVID-19 Test | USA | 83.5% | 99.2% | 90.0% | 1.9×104
TCID50/mL |
| BD Veritor System for Rapid Detection of SARS-CoV-2 | USA | 84% | 100.0% | 96.0% | 800 genomic RNA copies/ml |
| Roche Rapid Antigen Test | Germany | 82.2% | 99.0% | 95.0% | 9.25×101.2 TCID50/mL |
| Abbott – Panbio COVID-19 Antigen Rapid Test | Germany | 75.5% | 94.9% | 90.0% | Viral loads > 106 copies/ml |
| Xiamen Boson Biotech – SARS-CoV-2 Antigen Test Card | China | 96.5% | 99.0% | 98.7% | 130
TCID50/ml |
| Empowered Diagnostics CovClear COVID-19 Rapid Antigen Test | USA | 95.5% | 100.0% | 96.7% | 1.29×105 TCID50/ml |
* Sensitivity is a metric defining a test’s capacity to correctly identify people that are infected with SARS-CoV-2 when a test is positive. For example, a test with a sensitivity of 96% will, on average, correctly identify 96 people in every 100 who are truly infected with SARS-CoV-2.
** Specificity is a metric defining a test’s capacity to correctly identify people that are not infected with SARS-CoV-2 when a test is negative. For example, a test with a specificity of 96% will, on average, correctly identify 96 people in every 100 who are truly not infected with SARS-CoV-2.
*** Overall agreement: is the product of the equation: true positives + true negatives / total samples.
References
- Pegu A, O’Connell SE, Schmidt SD, O’Dell S, Talana CA, Lai L, et al. Durability of mRNA-1273 vaccine–induced antibodies against SARS-CoV-2 variants. Science. 2021;373(6561):1372-7.
- Naaber P, Tserel L, Kangro K, Sepp E, Jürjenson V, Adamson A, et al. Dynamics of antibody response to BNT162b2 vaccine after six months: a longitudinal prospective study. Lancet Reg Health Eur. 2021;10:100208.
- Zhang A, Breznik JA, Clare R, Nazy I, Miller MS, Bowdish DME, et al. Antibody Responses to Third-Dose mRNA Vaccines in Nursing Home and Assisted Living Residents. J Am Med Dir Assoc. 2022.
- Wölfel R, Corman VM, Guggemos W, Seilmaier M, Zange S, Müller MA, et al. Virological assessment of hospitalized patients with COVID-2019. Nature. 2020;581(7809):465-9.
- Bekliz M, Perez-Rodriguez F, Puhach O, Adea K, Melancia SM, Baggio S, et al. Sensitivity of SARS-CoV-2 antigen-detecting rapid tests for Omicron variant. medRxiv. 2022:2021.12.18.21268018.
- Sheikh A KS, Woolhouse M, McMenamin J, Robertson C. Severity of Omicron variant of concern and vaccine effectiveness against symptomatic disease: national cohort with nested test negative design study in Scotland. 2021 Dec 22.
- Wolter N, Jassat W, Walaza S, Welch R, Moultrie H, Groome M, et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: a data linkage study. Lancet. 2022.
- Abu-Raddad LJ, Chemaitelly H, Bertollini R. Severity of SARS-CoV-2 Reinfections as Compared with Primary Infections. N Engl J Med. 2021;385(26):2487-9.